Schizophrenia is a complex psychiatric disorder characterized by positive, negative, and cognitive symptoms. The dopamine hypothesis of schizophrenia posits that hyperactivity of dopamine pathways, particularly in the mesolimbic pathway, contributes to the positive symptoms of the illness. Antipsychotic medications, the primary pharmacological treatment for schizophrenia, exert their therapeutic effects largely through modulation of dopamine neurotransmission. This document explores the mechanisms by which antipsychotic drugs affect dopamine pathways. Both first-generation antipsychotics (FGAs) and second-generation antipsychotics (SGAs) primarily act as dopamine receptor antagonists, blocking dopamine receptors, particularly the D2 receptor subtype. However, SGAs exhibit a more complex pharmacological profile, often including serotonin receptor antagonism (e.g., 5-HT2A) in addition to dopamine receptor blockade. This serotonin antagonism is thought to contribute to the improved side effect profile and efficacy against negative symptoms observed with some SGAs. The document further examines the regional specificity of antipsychotic effects on dopamine release and metabolism, considering the mesolimbic, mesocortical, nigrostriatal, and tuberoinfundibular pathways. Understanding these mechanisms is crucial for optimizing antipsychotic treatment strategies, minimizing adverse effects such as extrapyramidal symptoms (EPS) and hyperprolactinemia, and developing novel therapeutic interventions targeting dopamine and other neurotransmitter systems in schizophrenia.
| Published in | International Journal of Medical Research and Innovation (Volume 1, Issue 1) |
| DOI | 10.11648/j.ijmri.20250101.16 |
| Page(s) | 47-52 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Antipsychotic, Schizophrenia, Dopamine, First Generation Antipsychotic Drugs, Second Generation Antipsychotic Drugs
Feature | First Antipsychotics Generation | Second Generation Antipsychotics |
|---|---|---|
Mechanism | Strong D2 blockage | D2 +5-HT2A antagonism |
EPS Risk | High | Low |
Metabolic Effects | Low | High |
Sedation | High in low-potency types | Moderate to High |
Prolactin | Common | Less common (risperidone) |
Example | Haloperidol, Chlorpromazine | Risperidone, Clozapine, Olanzapine |
| [1] | Oliver D Howes, Shitij Kapur. The dopamine hypothesis of schizophrenia: version III--the final common pathway |
| [2] | An umbrella review of adverse effects associated with antipsychotic medications: the need for complementary study designs Rachel T. S. Chow Seena Fazel. |
| [3] | Alpert NM, Badgaiyan RD, Livni E, Fischman AJ (2003). A novel method for noninvasive detection of neuromodulatory changes in specific neurotransmitter systems. NeuroImage 19: 1049–1060. |
| [4] | Arnsten AF, Cai JX, Steere JC, Goldman-Rakic PS (1995). Dopamine D2 receptor mechanisms contribute to age-related cognitive decline: the effects of quinpirole on memory and motor performance in monkeys. J Neurosci 15: 3429–3439. |
| [5] | Bartlett SE, Enquist J, Hopf FW, Lee JH, Gladher F, Kharazia V et al (2005). Dopamine responsiveness is regulated by targeted sorting of D2 receptors. Proc Natl Acad Sci USA 102: 11521–11526. |
| [6] | Beaulieu J-M, Del’ Guidice T, Sotnikova T, Lemasson M, Gainetdinov R (2011). Beyond cAMP: the regulation of Akt and GSK3 by dopamine receptors. Front Mol Neurosci 4: 38. |
| [7] | Beaulieu J-M, Gainetdinov RR (2011). The physiology, signaling, and pharmacology of dopamine receptors. Pharmacol Rev 63: 182–217. |
| [8] | Bhattacharyya S, Raote I, Bhattacharya A, Miledi R, Panicker MM (2006). Activation, internalization, and recycling of the serotonin 2A receptor by dopamine. Proc Natl Acad Sci USA 103: 15248–15253. |
| [9] | Bolaños-Jiménez R, Arizmendi-Vargas J, Martínez-Zavala N, Carrillo-Ruiz J, Damián CÁ-TJ, Luis J-PF et al (2011). Quinpirole effects on the dopaminergic system. Br J Pharmacol Toxicol 2: 310. |
| [10] | Breier A, Su T-P, Saunders R, Carson RE, Kolachana BS, de Bartolomeis A et al (1997). Schizophrenia is associated with elevated amphetamine-induced synaptic dopamine concentrations: Evidence from a novel positron emission tomography method. Proc Natl Acad Sci USA 94: 2569–2574. |
| [11] | Carson RE, Channing MA, Blasberg RG, Dunn BB, Cohen RM, Rice KC et al (1993). Comparison of bolus and infusion methods for receptor quantitation: application to [18f]cyclofoxy and positron emission tomography. J Cereb Blood Flow Metab 13: 24–42. |
| [12] | Catana C, van der Kouwe A, Benner T, Michel CJ, Hamm M, Fenchel M et al (2010). Toward implementing an MRI-based PET attenuation-correction method for neurologic studies on the MRPETbrain prototype. J Nucl Med 51: 1431–1438. |
| [13] | Chen YCI, Galpern WR, Brownell AL, Matthews RT, Bogdanov M, Isacson O, et al. Detection of dopaminergic neurotransmitter activity using pharmacologic MRI: correlation with PET, microdialysis, and behavioral data. Magn Reson Med. 1997; 38: 389–398. |
| [14] | Neuroreport 10: 2881–2886. Choi J-K, Chen YI, Hamel E, Jenkins BG (2006). Brain hemodynamic changes mediated by dopamine receptors: role of the cerebral microvasculature in dopamine-mediated neurovascular coupling. NeuroImage 30: 700–712. |
| [15] | Chugani DC, Ackermann RF, Phelps ME (1988). In vivo [3H]spiperone binding: evidence for accumulation in corpus striatum by agonist-mediated receptor internalization. J Cereb Blood Flow Metab 8: 291–303. |
| [16] | Clark AJ (1937). General Pharmacology. Springer-Verlag: Berlin, New York. |
| [17] | Coldwell MC, Boyfield I, Brown T, Hagan JJ, Middlemiss DN (1999). Comparison of the functional potencies of ropinirole and other dopamine receptor agonists at human D2(long), D3 and D4.4 receptors expressed in Chinese hamster ovary cells. Br J Pharmacol 127: 1696–1702. |
| [18] | Cox RW (2012). AFNI: what a long strange trip it’s been. Neuroimage 62: 743–747. |
| [19] | Cumming P (2011). Absolute abundances and affinity states of dopamine receptors in mammalian brain: a review. Synapse 65: 892–909. |
| [20] | Eilam D, Szechtman H (1989). Biphasic effect of D-2 agonist quinpirole on locomotion and movements. Eur J Pharmacol 161: 151–157. |
| [21] | Gardner B, Strange PG (1998). Agonist action at D2(long) dopamine receptors: ligand binding and functional assays. Br J Pharmacol 124: 978–984. Ginovart N (2005). |
| [22] | Imaging the dopamine system with in vivo [11C]raclopride displacement studies: understanding the true mechanism. Mol Imaging Biol 7: 45–52. |
| [23] | Delay J, Deniker P, Harl JM. Therapeutic use in psychiatry of phenothiazine of central elective action (4560 RP) Ann Med Psychol (Paris) 1952; 110: 112–117. |
| [24] | Carlsson A, Lindqvist M, Magnusson T. 3,4-Dihydroxyphenylalanine and 5-hydroxytryptophan as reserpine antagonists. Nature. 1957; 180: 1200. |
| [25] | Lieberman JA, Kane JM, Alvir J. Provocative tests with psychostimulant drugs in schizophrenia. Psychopharmacology (Berl) 1987; 91: 415–433. |
| [26] | Seeman P, Lee T. Antipsychotic drugs: direct correlation between clinical potency and presynaptic action on dopamine neurons. Science. 1975; 188: 1217–1219. |
| [27] | Matthysse S. Antipsychotic drug actions: a clue to the neuropathology of schizophrenia? Fed Proc. 1973; 32: 200–205. |
| [28] | Snyder SH. The dopamine hypothesis of schizophrenia: focus on the dopamine receptor. Am J Psychiatry. 1976; 133: 197–202. |
| [29] | Davis KL, Kahn RS, Ko G, Davidson M. Dopamine in schizophrenia: a review and reconceptualization. Am J Psychiatry. 1991; 148: 1474–1486. |
| [30] | Pycock CJ, Kerwin RW, Carter CJ. Effect of lesion of cortical dopamine terminals on subcortical dopamine receptors in rats. Nature. 1980; 286: 74–76. |
| [31] | Scatton B, Worms P, Lloyd KG, Bartholini G. Cortical modulation of striatal function. Brain Res. 1982; 232: 331–343. |
| [32] | Davidson LL, Heinrichs RW. Quantification of frontal and temporal lobe brain-imaging findings in schizophrenia: a meta-analysis. Psychiatry Res. 2003; 122: 69–87. |
| [33] | McGuire P, Howes OD, Stone J, Fusar-Poli P. Functional neuroimaging in schizophrenia: diagnosis and drug discovery. Trends Pharmacol Sci. 2008; 29: 91–98. |
| [34] | Moore RY, Whone AL, McGowan S, Brooks DJ. Monoamine neuron innervation of the normal human brain: an 18F-DOPA PET study. Brain Res. 2003; 982: 137–145. |
| [35] | Meyer-Lindenberg A, Miletich RS, Kohn PD, et al. Reduced prefrontal activity predicts exaggerated striatal dopaminergic function in schizophrenia. Nat Neurosci. 2002; 5: 267–271. |
APA Style
Muskan, V. (2025). Dopamine Modulation by Antipsychotic in Schizophrenia. International Journal of Medical Research and Innovation, 1(1), 47-52. https://doi.org/10.11648/j.ijmri.20250101.16
ACS Style
Muskan, V. Dopamine Modulation by Antipsychotic in Schizophrenia. Int. J. Med. Res. Innovation 2025, 1(1), 47-52. doi: 10.11648/j.ijmri.20250101.16
AMA Style
Muskan V. Dopamine Modulation by Antipsychotic in Schizophrenia. Int J Med Res Innovation. 2025;1(1):47-52. doi: 10.11648/j.ijmri.20250101.16
@article{10.11648/j.ijmri.20250101.16,
author = {Verma Muskan},
title = {Dopamine Modulation by Antipsychotic in Schizophrenia},
journal = {International Journal of Medical Research and Innovation},
volume = {1},
number = {1},
pages = {47-52},
doi = {10.11648/j.ijmri.20250101.16},
url = {https://doi.org/10.11648/j.ijmri.20250101.16},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijmri.20250101.16},
abstract = {Schizophrenia is a complex psychiatric disorder characterized by positive, negative, and cognitive symptoms. The dopamine hypothesis of schizophrenia posits that hyperactivity of dopamine pathways, particularly in the mesolimbic pathway, contributes to the positive symptoms of the illness. Antipsychotic medications, the primary pharmacological treatment for schizophrenia, exert their therapeutic effects largely through modulation of dopamine neurotransmission. This document explores the mechanisms by which antipsychotic drugs affect dopamine pathways. Both first-generation antipsychotics (FGAs) and second-generation antipsychotics (SGAs) primarily act as dopamine receptor antagonists, blocking dopamine receptors, particularly the D2 receptor subtype. However, SGAs exhibit a more complex pharmacological profile, often including serotonin receptor antagonism (e.g., 5-HT2A) in addition to dopamine receptor blockade. This serotonin antagonism is thought to contribute to the improved side effect profile and efficacy against negative symptoms observed with some SGAs. The document further examines the regional specificity of antipsychotic effects on dopamine release and metabolism, considering the mesolimbic, mesocortical, nigrostriatal, and tuberoinfundibular pathways. Understanding these mechanisms is crucial for optimizing antipsychotic treatment strategies, minimizing adverse effects such as extrapyramidal symptoms (EPS) and hyperprolactinemia, and developing novel therapeutic interventions targeting dopamine and other neurotransmitter systems in schizophrenia.},
year = {2025}
}
TY - JOUR T1 - Dopamine Modulation by Antipsychotic in Schizophrenia AU - Verma Muskan Y1 - 2025/12/17 PY - 2025 N1 - https://doi.org/10.11648/j.ijmri.20250101.16 DO - 10.11648/j.ijmri.20250101.16 T2 - International Journal of Medical Research and Innovation JF - International Journal of Medical Research and Innovation JO - International Journal of Medical Research and Innovation SP - 47 EP - 52 PB - Science Publishing Group SN - 3070-6319 UR - https://doi.org/10.11648/j.ijmri.20250101.16 AB - Schizophrenia is a complex psychiatric disorder characterized by positive, negative, and cognitive symptoms. The dopamine hypothesis of schizophrenia posits that hyperactivity of dopamine pathways, particularly in the mesolimbic pathway, contributes to the positive symptoms of the illness. Antipsychotic medications, the primary pharmacological treatment for schizophrenia, exert their therapeutic effects largely through modulation of dopamine neurotransmission. This document explores the mechanisms by which antipsychotic drugs affect dopamine pathways. Both first-generation antipsychotics (FGAs) and second-generation antipsychotics (SGAs) primarily act as dopamine receptor antagonists, blocking dopamine receptors, particularly the D2 receptor subtype. However, SGAs exhibit a more complex pharmacological profile, often including serotonin receptor antagonism (e.g., 5-HT2A) in addition to dopamine receptor blockade. This serotonin antagonism is thought to contribute to the improved side effect profile and efficacy against negative symptoms observed with some SGAs. The document further examines the regional specificity of antipsychotic effects on dopamine release and metabolism, considering the mesolimbic, mesocortical, nigrostriatal, and tuberoinfundibular pathways. Understanding these mechanisms is crucial for optimizing antipsychotic treatment strategies, minimizing adverse effects such as extrapyramidal symptoms (EPS) and hyperprolactinemia, and developing novel therapeutic interventions targeting dopamine and other neurotransmitter systems in schizophrenia. VL - 1 IS - 1 ER -
Saraswati Institute of Pharmaceutical Sciences, Gandhinagar, India
Figure 1. Neural circuitry involved in dopamine regulation and its relevance to schizophrenia.
Figure 2. Relationship between dopamine dysregulation, clinical symptoms, and antipsychotic medication effects in schizophrenia.
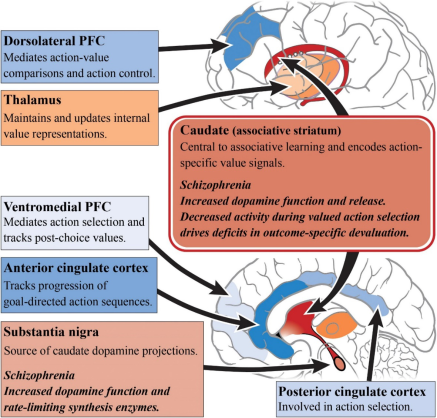
Figure 3. Classification of antipsychotic medications showing major categories and overlapping pharmacological properties.

